Untested bivalent COVID jab being rolled out
09/19/2022 / By News Editors

STORY AT-A-GLANCE
- August 15, 2022, the U.K. became the first country to approve Moderna’s new bivalent COVID booster — Spikevax bivalent — which contains mRNA that codes for the original Wuhan strain spike protein and the Omicron BA.1 subvariant
- The approval of the new booster comes on the heels of complaints about lack of demand for the shots. Moderna recently threw away 30 million doses of its original COVID jab, as nobody wanted them, and the U.S., has tossed 82.1 million COVID jab doses in the trash for the same reason
- The Spikevax bivalent shot is already out of date, as both strains included are no longer in circulation anywhere in the world
- In the U.S., infections are currently caused by the BA.4, BA.5 and BA.2.12.1 variants of Omicron. In Europe, Omicron BA.2, BA.4 and BA.5 are the current “variants of concern.” BA.1 is on the list of “de-escalated variants,” meaning it’s of no concern either because it’s either not in circulation, or because it doesn’t cause severe illness
- Coronaviruses mutate very rapidly, and when you vaccinate against a rapidly mutating virus, you encourage it to mutate even faster, and to develop immune-evading properties. This is what we’ve been witnessing since the beginning of the COVID jab campaign, and outdated, leaky bivalent boosters may worsen the situation further
(Article by Dr. Joseph Mercola republished from Articles.Mercola.com)
August 15, 2022, the U.K. became the first country to approve Moderna’s new bivalent COVID booster, which contains both the original concoction and mRNA to target Omicron variants. The booster has also been submitted for approval with authorities in Australia, Canada and the EU, and there’s every reason to suspect it’ll be submitted to the U.S. Food and Drug Administration as well. As reported by Sky News:1
“The booster dose, known as ‘Spikevax bivalent Original/Omicron,’ contains 25 micrograms of Omicron vaccine and 25 micrograms of original coronavirus vaccine …
The Joint Committee on Vaccination and Immunization (JCVI) has said the vaccine will be available to those aged 18 and over as part of the UK’s autumn booster program. Health Secretary Steve Barclay said those eligible will be contacted from early September.”
More Than 100 Million Doses Have Been Trashed
The approval of the new booster comes right on the heels of widespread complaints about lack of demand for the shots. Moderna recently had to throw away 30 million doses of its original COVID jab, as there was no demand for them.2
“We have a big demand problem,” Moderna CEO Stéphane Bancel said in May 2022 during a panel discussion at the World Economic Forum’s meeting in Davos, Switzerland.3 Similarly, in the U.S., pharmacies, states and federal agencies have tossed 82.1 million COVID jab doses in the trash, and for the same reason.4
Bivalent Booster Is Already Out of Date
Moderna’s bivalent booster is said to “provide a strong immune response against the Omicron BA.1 variant as well as the original 2020 Wuhan strain,” which, for the record, is extinct and no longer in circulation anywhere in the world. BA.1 is now rarely ever found, either.
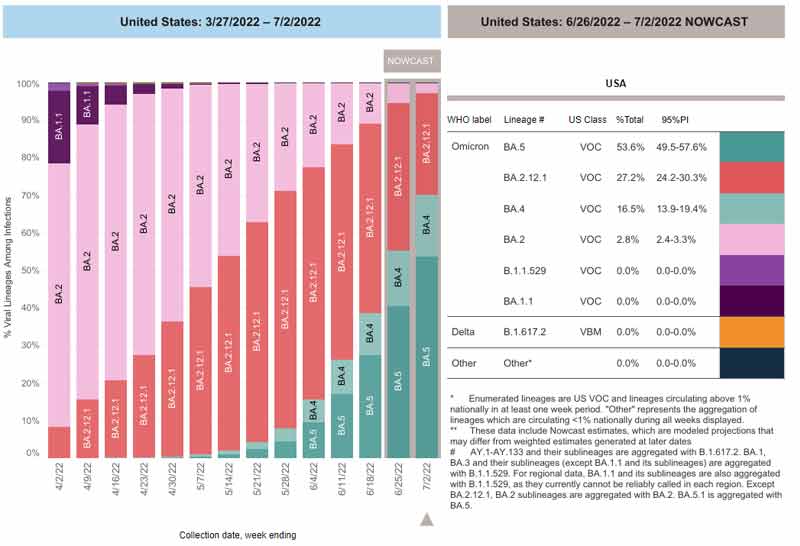
The graph5,6 below, from the U.S. Centers for Disease Control and Prevention, shows the infection ratios of common variants. As you can see, in the U.S., infections are now caused by the BA.4, BA.5 and BA.2.12.1 variants of Omicron.7 So, this booster contains two strains that aren’t even relevant anymore.
The situation is exactly the same in Europe, where Omicron BA.2, BA.4 and BA.5 are the current “variants of concern.” BA.1 isn’t even a “variant of interest,” which is the next-lower categorization. It’s on the list of “de-escalated variants,” which is based on a variant meeting one or more of the following criteria:8
“(1) the variant is no longer circulating, (2) the variant has been circulating for a long time without any impact on the overall epidemiological situation, (3) scientific evidence demonstrates that the variant is not associated with any concerning properties.”
In short, BA.1 is of no concern in Europe either, as it’s not in circulation and/or because it doesn’t cause severe illness. The same goes for the original Wuhan strain, which has long since mutated out of existence.
Vaccinating Against Rapidly Mutating Viruses Is a Bad Idea
Coronaviruses mutate very rapidly in general, and the mRNA jabs are based on a surface protein (the spike protein), which is the most rapidly mutating portion of the entire virus. What happens when you vaccinate against a rapidly mutating virus? You encourage it to mutate even faster, and to develop immune-evading properties.
This is what we’ve been witnessing since the beginning of the COVID jab campaign, and at this point, there’s no hope of ever catching up with the virus. What’s worse, while variants have so far evolved into milder strains, they are in fact gaining the ability to evade antibodies, and could theoretically switch course to become more pathogenic.9
This is particularly true when a vaccine is “leaky,” meaning it doesn’t fully prevent infection (which none of the COVID shots do). Just like when you overuse an antibiotic that fails to eradicate the bacteria, which allows antibiotic-resistant bacteria to flourish, overuse of a leaky vaccine can pressure a virus to become more lethal.10,11
BA.4 and BA.5 are the most resistant to date, with BA.5 circumventing the immune systems even of those with natural immunity.12 Fortunately, it doesn’t appear to cause severe illness in most people.
The take-home here is that had natural immunity been allowed to take place without these jabs, the pandemic would be over and reinfections near-nonexistent. Instead, we’re now in a pandemic of the vaccinated, with the vast majority of serious COVID infections occurring among those who have been jabbed.13,14
We know that Pfizer was aware of this possibility, as “vaccine-associated enhanced disease (VAED)” is listed as an “Important Potential Risk” in Table 5 on page 11 of a document called “5.3.6 Cumulative Analysis of Post-Authorization Adverse Event Reports.”15 This document was part of the FOIA required and court-ordered batch released by the FDA April 1, 2022.
How Long Will the Bivalent Booster Protect You?
According to Moderna, the bivalent Spikevax “demonstrates potent neutralizing antibody response against Omicron subvariants BA.4 and BA.5.”16 They made the same claim for the original COVID jab, back in January 2021,17 and by August 2021, they admitted the neutralizing antibodies generated lasted only six months after the second dose.18
How long will the bivalent jab “be effective” (and I use that term loosely)? Who knows, but the way things are trending, six months would probably be the max. In Germany, citizens must now get a booster every three months to qualify as “fully vaccinated,”19 as rapidly waning immunity has become accepted fact, and that’s probably where we’re all headed.
Germans who haven’t received all of their boosters will be subject to mask mandates and other COVID restrictions this fall. This, despite deep criticism from businesses tasked with confirming their customers’ status. As reported by the Rise Align Ignite Reclaim (RAIR) foundation:20
“Businesses have voiced great concern about further regulatory chaos in the struggling economy. ‘The plans are simply not feasible,’ said the general manager of the German Hotel and Restaurant Association (Dehoga), Ingrid Hartges, the Handelsblatt. ‘We cannot constantly check whether our guests are vaccinated, recovered, or tested.’
These people are exempted from the obligation to wear masks in restaurants or events under certain circumstances — if the vaccination, for example, is within the last three months. ‘But you can’t tell from the guest in the restaurant what status they have,’ says Hartges. ‘Like when he goes to the bathroom — should the staff always ask if he’s vaccinated?’ she said. ‘That’s nonsense.'”
Bivalent Jab Will Not Undergo Additional Testing
It’s important to realize that these “next-gen” boosters will not undergo any additional safety testing.21,22 They’re being rolled out under a new fast-track standard where ingredients can be swapped out without additional testing.
This is the standard protocol for seasonal flu vaccines. However, we’re now using an entirely new type and essentially untested technology. There’s no telling whether variations in the spike mRNA being injected might produce vastly differing side effects. They could potentially have differing toxicities, but that’s not being investigated.
Also, remember that the “efficacy” they’re referring to is only based on measurements of antibody titers, which tells us nothing, really, about its ability to prevent infection, severity of illness or death. Why?
Because antibodies form only a part of your immune response, and they’re not even the most important. It is far more likely that your innate immune system — your first line of defense — will destroy a virus before your adaptive immune system even has a chance to respond and create antibodies.23
It is important to understand that no vaccine improves your innate immune response. All vaccines are ever able to do is address your adaptive humoral immune system and create antibodies. Your innate immune system has T cells that can directly kill viruses. If you happen to have a vigorous T cell response, you’ll be protected even if your antibodies are low. So, antibodies are not a necessary measure of immunity.
Antibody titer levels are what’s called a “surrogate outcome.” It’s a substitute for actual clinical outcome. But it’s in no way equivalent, no matter how much the powers in control want it to be. Antibody titers may be high, but in the real world, more people may end up in the hospital and die — either from the infection or from the shot. In short, high antibody titer is not a guarantee of effectiveness — and it tells us absolutely nothing about safety.
CIA-Backed Upstart to Produce Moderna’s Bivalent mRNA
The complete absence of testing moving forward is all the more concerning when you consider who’s manufacturing the RNA for Moderna’s now-bivalent booster. In a recent Unlimited Hangout article,24 investigative journalist Whitney Webb reveals the genetic material for the reformulated booster is being exclusively manufactured by National Resilience, a relative newcomer with significant ties to U.S. intelligence agencies.
Its board of directors include In-Q-Tel CEO Chris Darby, who is also on the board of directors of the CIA Officers Memorial Foundation, and former FDA commissioner and Pfizer board member Dr. Scott Gottlieb. Not surprisingly, National Resilience promises to successfully lead its customers through the government regulatory process. As reported by Webb:25
“National Resilience was founded … in November 2020, and … plans to ‘reinvent biomanufacturing’ and democratize access to medicines,’ namely gene therapies, experimental vaccines and other ‘medicines of tomorrow’ …
In April 2021, National Resilience acquired Ology Bioservices Inc., which had received a $37 million contract from the US military the previous November to develop an advanced anti-COVID-19 monoclonal antibody treatment. This acquisition also provided National Resilience with its first Biosafety Level 3 (BSL-3) laboratory and the ability to manufacture cell and gene therapies, live viral vaccines and vectors and oncolytic viruses.
Despite being in the earliest stages of developing its ‘revolutionary’ manufacturing capabilities, National Resilience entered into a partnership with the Government of Canada in July of last year. Per that agreement, the Canadian government plans to invest CAD 199.2 million (about $154.9 million) into National Resilience’s Ontario-based subsidiary, Resilience Biotechnologies Inc.
Most of those funds are destined for use in expanding the Ontario facility that Resilience acquired last March and which is now manufacturing the mRNA for Moderna’s COVID-19 products … More recently, in 2022, the company has announced a few new clients – Takeda, Opus Genetics and the US Department of Defense …
Considering Moderna’s history and Resilience’s connections, there may be more to this partnership that meets the eye and concerned members of the public would do well to keep a very close eye on Resilience, its partnerships, and the products it is manufacturing.
Given that we now live in a world where government regulatory decisions on the approval of medicines are increasingly influenced by corporate press releases and normal regulatory procedures have fallen by the wayside for being too ‘slow,’ there is likely to be little scrutiny of the genetic material that Resilience produces for the ‘medicines of tomorrow.’
This seems to be already true for Moderna’s recently retooled COVID-19 vaccine, as there has been no independent examination of the new genetic sequence of mRNA used in the Omicron-specific vaccine candidate or its effects on the human body in the short, medium or long term.
For those who are skeptical of the outsized role that intelligence-linked companies are playing in the attempted technological ‘revolution’ in the medical field, it is best to consider Resilience’s role in the upcoming fall vaccination campaign and in future pandemic and public health scenarios before trying its ‘futuristic’ products.”
Was COVID Jab Intentionally Flawed?
In a June 2022 interview with British radio presenter Maajid Nawaz, Michael Yeadon, Ph.D., a former vice-president and chief scientific adviser for Pfizer and founder/CEO of the biotech company Ziarco (now owned by Novartis), explained why he believes the COVID jabs were intentionally made to be harmful and to prolong the pandemic.
For starters, it’s been known for more than 10 years that spike protein causes adverse effects in humans,26 so this could not be a design error. It must have been intentional.
As Yeadon explained, when making a vaccine, you have to be very careful about which part of the virus you use, as certain parts are more toxic and some provoke better immune responses than others. “What you would do is ask, ‘What’s the toxicity of the bit I’m going to give a person?'” he said.
Seeing how scientists have known for at least a decade that spike protein from related viruses causes blood clots through at least two different mechanism, the choice to use mRNA that programs your cells to make spike protein raised a warning flag from the start.
Nothing About the COVID Jabs Makes Sense
In addition to that, 90% of the immune response you get from natural COVID infection is in response to other parts of the virus, not the spike protein. Put another way, exposure to spike protein mounts an inferior immune response. If you’re looking to make an effective vaccine, wouldn’t you choose a part of the virus that mounts the best and most robust immune response?
By choosing the spike protein on which to base COVID-19 shots, scientists picked a protein that a) was known to be toxic to humans and b) produced an inferior immune response (compared to other parts of the virus).
On top of that, spike protein mutates rapidly, which destroys any protection the shot provides shortly after it’s given. As noted by Yeadon,27 “What you should do is pick the bits of the virus that’s genetically most stable,” but they didn’t do that. Why not? The end result is a seemingly never-ending series of boosters, and according to Yeadon, that may have been the plan from the start.
As if all of that weren’t enough, the spike protein is also similar to a variety of human proteins, which can trigger your body to mount an inappropriate immune response against your own proteins. In other words, it can cause autoimmune disease. Yet, scientists chose the spike protein anyway — even though it violated all of the accepted rules for creating a safe and effective product.
Collusion to Cause Harm
Yeadon believes the decision to use spike protein was not a mistake at all. He believes it was intentionally chosen because it has all of those ill effects. He told Nawaz:
“Again, you deselect things that are toxic in their own right, you pick things that are genetically stable, and you pick things that are most different from humans …
But guess what? Moderna picks spike protein and so does Pfizer, and AstraZeneca, and Johnson & Johnson. So, I put it to you, colleagues, any scientists out there or just logical people. How the hell would they pick [the spike protein]?
No team I was ever part of would ever have picked bloody spike protein for this vaccine. And you know what? If we did, and we have competing groups, we would not, all four of us, make the same mistake. Not possible. It’s collusion and malfeasance. The did it on purpose, knowing it would hurt you.”
Resources for Those Injured by the COVID Jabs
If you got one or more jabs and suffered an injury, first and foremost, never ever take another COVID booster, another mRNA gene therapy shot or regular vaccine. You need to end the assault on your system. The same goes for anyone who has taken one or more COVID jabs and had the good fortune of not experiencing debilitating side effects.
Your health may still be impacted long-term, so don’t take any more shots. When it comes to treatment, there are still more questions than answers, and most doctors are clueless about what to do — in part because they never bothered to give early treatment for COVID and therefore don’t understand how different medicines and supplements impact the spike protein.
So far, it seems like many of the treatments that worked against severe COVID-19 infection also help ameliorate adverse effects from the jab. This makes sense, as the toxic, most damaging part of the virus is the spike protein, and that’s what your whole body is producing if you got the jab.
Two doctors who have started tackling the treatment of COVID jab injuries in earnest include Dr. Michelle Perro (DrMichellePerro.com), whom I’ve interviewed on this topic, and Dr. Pierre Kory (DrPierreKory.com).
Both agree that eliminating the spike protein your body is now continuously producing is a primary task. Perro’s preferred remedy for this is hydroxychloroquine, while Kory typically uses ivermectin. Both of these drugs bind and thereby facilitate the removal of spike protein.
Kory also believes there may be ways to boost the immune system to allow it to degrade and eventually remove the spike from your cells naturally, over time. One of the strategies he recommends for this is TRE (time restricted eating), which stimulates autophagy, a natural cleaning process that eliminates damaged, misfolded and toxic proteins. Another strategy that can do the same thing would be sauna therapy.
As a member of the Front Line COVID-19 Critical Care Alliance (FLCCC), Kory helped develop the FLCCC’s post-vaccine treatment protocol called I-RECOVER. Since the protocol is continuously updated as more data become available, your best bet is to download the latest version straight from the FLCCC website at covid19criticalcare.com28 (hyperlink to the correct page provided above).
Other Helpful Treatments and Remedies
In previous articles, I’ve also covered a number of treatments and remedies that can be helpful for COVID jab injuries, such as:
- Hyperbaric oxygen therapy, especially in cases involving stroke, heart attack, autoimmune diseases and/or neurodegenerative disorders. To learn more, see “Hyperbaric Therapy — A Vastly Underused Treatment Modality.”
- Lower your Omega-6 intake. Linoleic acid is consumed in amounts ten times of ideal in well over 95% of the population, and contributes to massive oxidative stress that impairs your immune response. Seed oils and processed foods need to be diligently avoided. You can review my previous post for more information.
- Time Restricted Eating will go a long way to decrease insulin resistance and improve metabolic flexibility. Most people eat more than 12 hours a day. The ideal window for most everyone is 16 to 18 hours of continuous fasting with last meal at least three hours before bed. If you are overweight, it’s best to shoot for 18 hours; if you’re of normal weight, 16 hours.
- Pharmaceutical grade methylene blue, which improves mitochondrial respiration and aid in mitochondrial repair. At 15 to 80 milligrams a day for those suffering from long-haul COVID could go a long way toward resolving some of the fatigue many suffer post-jab. Methylene blue is actually the parent molecule for hydroxychloroquine and has been used to treat malaria since 1890.
- It may also be helpful in acute strokes. The primary contraindication is if you have a G6PD deficiency (a hereditary genetic condition), in which case you should not use methylene blue at all. To learn more, see “The Surprising Health Benefits of Methylene Blue.”
- Near-infrared light, as it triggers production of melatonin in your mitochondria29 where you need it most. By mopping up reactive oxygen species, it too helps improve mitochondrial function and repair. Natural sunlight is 54.3% infrared radiation,30 so this treatment is available for free. For more information, see “What You Need to Know About Melatonin.”
Read more at: Articles.Mercola.com
Submit a correction >>
Tagged Under:
big government, Big Pharma, booster, Censored Science, chemical violence, Collusion, conspiracy, COVID, deception, depopulation, health, Medical Tyranny, medical violence, Moderna, mRNA, pandemic, pharmaceutical fraud, science deception, vaccine, vaccine death, vaccine injury, vaccines
This article may contain statements that reflect the opinion of the author
RECENT NEWS & ARTICLES